
by Derek Baughman, MD; Salma Green, DO; and Abdul Waheed, MD, MS, FAAFP
WellSpan Good Samaritan Hospital Family Medicine Residency Program, Lebanon PA
Background
As a core Accreditation Council for Graduate Medical Education (ACGME) accreditation requirement for residency programs, continuity clinic forms the foundation for competence in outpatient family medicine and is a practice focus of most graduates. The Association of Family Medicine Residency Directors’ Clinic First Collaborative1 is a popular conceptual model of achieving this foundational goal. Although many residency programs have adopted a clinic-first model, there is limited literature detailing the implementation of such scheduling models. Thus, we outline a high-yield Continuity-Clinic-Centered (C-3) scheduling model that is simple to implement.
Problem
Resident scheduling is complex due to multiperiod assignments and multiple constraints, including ACGME work-hour regulations and demanding coverage of the residency program’s inpatient services.2,3 For example, an analysis of scheduling complexity for a 24-resident family medicine (FM) program with only nine annual rotations resulted in more than 3,000 variables and more than 850 constraints3 Programs embracing a C-3 model can produce higher quadruple-aim care and have been endorsed by national organizations.4 Studies on FM residencies embracing these models have shown the feasibility of tackling complex scheduling with a two-pronged approach: separate master block schedules for core rotations and continuity clinics.5 The literature has highlighted the superiority of automated approaches to residency scheduling6 due to its ability to decrease drafting time,7 increase schedule quality,7,8 and improve resident satisfaction.8
Intervention
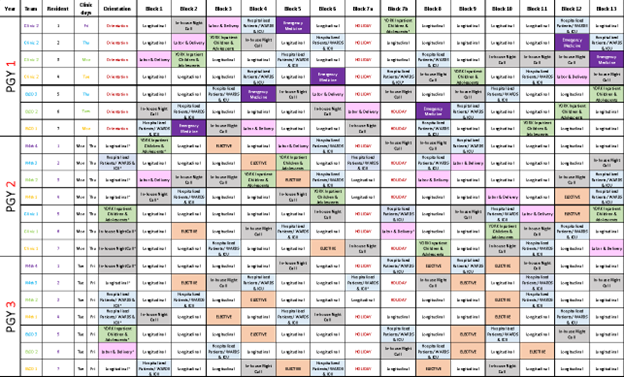
Our 7-7-7 FM residency program utilized schedule templates constructed in hierarchical stages by postgraduate year (PGY). Starting with designated resident clinic days for each PGY class, we established a clinic team template (Table 1). A separate template (Table 2) designated alternate days to coordinate residents on hospital service rotations. Subsequently, a 13-block hospital service and longitudinal subspecialty rotation block schedule (Figure 1) was constructed (separate Microsoft Excel sheets built specific longitudinal subspecialty rotation blocks and continuity clinics). The Excel “countif” function confirmed accuracy and fairness of resident block schedules facilitating a threefold tabulation: (1) even numbers of resident core rotations, longitudinal blocks, vacation and electives; (2), even numbers of subspecialty rotations; (3) a balance of preceptors, clinical staff, and provider availability at clinics.
Impact
The automated Excel spreadsheets facilitated predictable clinic schedules, enhanced resident empanelment, and promoted continuity of team-based care to fulfill the 1,650 outpatient visit requirement.9 This improved schedule coverage of 273 unique 2-week blocks of core rotations and clinic coverage for our 21 residents across three PGYs (Figure 1). Automation provided more efficient and accurate tabulation than prior hand-counting methods resulting in fewer scheduling mistakes throughout the academic year. Spreadsheets served as templates for subsequent academic years and significantly reduced both quantity and duration of scheduling meetings for administrative staff, chief residents, and program director.
Although automated cloud-based physician scheduling software was considered for our program, high implementation fees10 rendered this an unfeasible option given our residency budget. Alternatively, we found simple Excel formulas an affordable solution to ensure accuracy of the C-3 model. Additionally, Excel’s conditional formatting feature facilitated instant visualization of gaps, over- or undercoverage, and preceptor supersaturation. Making schedule changes with this method also avoided the need to manually recount blocks as “countif” works in real time. This was exceedingly helpful for quickly understanding the effects of multiple residents requesting vacation or CME conference attendance. Most importantly, this same method can be applied to the clinic block schedule ensuring prioritization of clinics and their C-3 coverage.
Conclusion
Clinic-first models for residency scheduling can be streamlined with simple templates that ensure fairness, balance, and reproducibility of resident scheduling. Automated templating with spreadsheet software is an evidence-based approach to navigate accreditation constraints and solve complex multiperiod assignments for residency programs.
Figures and Tables
Table 1: C-3 Model of Resident Team-Based Clinic
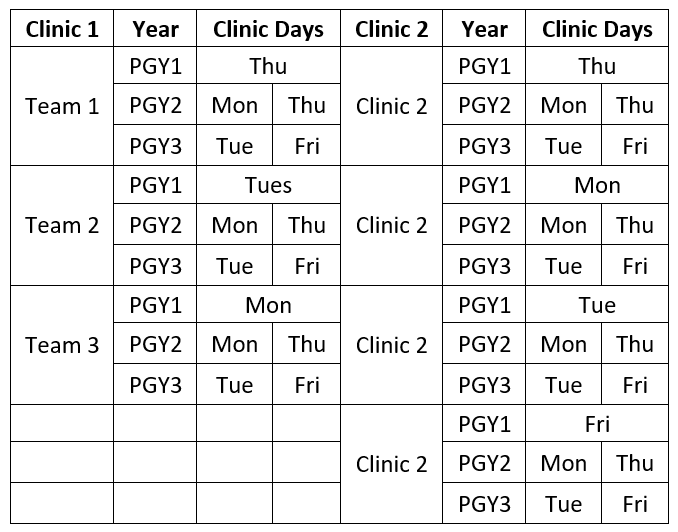
Table 2: C-3 Model for Hospital Service Rotations (Including Inpatient, OB, and Night Float)

Figure 1: C-3 Model Longitudinal Block Schedule by PGY
References
1. Topaloglu S, Ozkarahan I. A constraint programming-based solution approach for medical resident scheduling problems. Comput Oper Res. 2011;38(1):246-255. doi:10.1016/j.cor.2010.04.018
2. Franz LS, Miller JL. Scheduling Medical Residents to Rotations: Solving the Large-Scale Multiperiod Staff Assignment Problem. Oper Res. 1993;41(2):269-279. doi:10.1287/opre.41.2.269
3. AFMRD – Clinic First Collaborative. Association of Family Medicine Residency Directors. Accessed March 17, 2021. https://www.afmrd.org/page/clinicfirstcollaborative
4. Brown SR, Bodenheimer T, Kong M. High-performing primary care residency clinics: a collaboration. Ann Fam Med. 2019;17(5):470-471. doi:10.1370/afm.2452
5. Bard JF, Shu Z, Morrice DJ, Leykum LK, Poursani R. Annual block scheduling for family medicine residency programs with continuity clinic considerations. IIE Trans. 2016;48(9):797-811. doi:10.1080/0740817X.2015.1133942
6. Ito M, Onishi A, Suzuki A, Imamura A, Ito T. The resident scheduling problem: a case study at Aichi Medical University Hospital. Journal of Japan Industrial Management Association. 2018;68(4E):259-272. doi:10.11221/JIMA.68.259
7. Perelstein E, Rose A, Hong Y-C, Cohn A, Long MT. Automation improves schedule quality and increases scheduling efficiency for residents. J Grad Med Educ. 2016;8(1):45-49. doi:10.4300/JGME-D-15-00154.1
8. Howard FM, Gao CA, Sankey C. Implementation of an automated scheduling tool improves schedule quality and resident satisfaction. PLoS One. 2020;15(8):e0236952. doi:10.1371/journal.pone.0236952


