This is is part of the Pecha Kucha: A Special Families and Health Blog Series.

Valerie Ross, MS, LMFT
At age 9 I took up the cello. It has been one of the joys of my life and surprisingly an important influence in my approach to teaching physicians.
To learn to play an instrument, you perform in front of a teacher who uses everything they know to coach you to play proficiently and musically. They first listen, they demonstrate and teach specific skills like how to hold the instrument or draw the bow, asking questions and offering encouragement. Then you go home and practice and come back for more coaching.
Imagine for a moment if we taught musicians the way we teach most health care clinicians. A learner would rarely play their instrument in front of their teacher. They’d describe their perception of their playing. We’d learn how they think about playing their instrument but not how they actually play. It does not make sense to us to think about training musicians or athletes without observation and coaching, and yet this is the way many health care providers are taught. We need to define, hear, see, and model the concepts and skills we want our learners to practice.
As a family therapist and behavioral scientist in a family medicine residency, I regularly observe residents in clinical encounters; in this context I find opportunities to teach them about the family systems concept called triangulation.
Two founding fathers of a family-oriented primary care approach, Bill Doherty, PhD, and Mac Baird, MD, observed that the doctor-patient relationship is always a triangle involving the clinician, the patient, and the family.

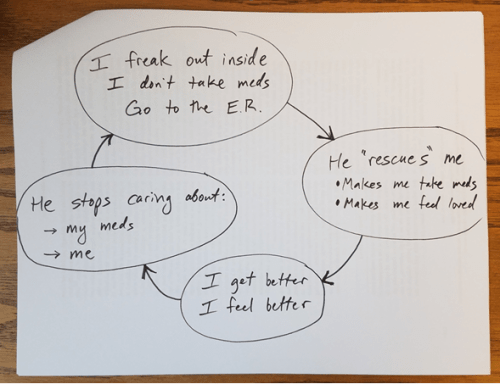
A clinician can use her or his position in the triangle therapeutically. However, if we are unaware of this triangle, we neglect to think about family members who are not in the room and we risk the possibility of unconscious “triangulation.”