
By La Donna Porter, MD, and Margaret Stafford, MD.
Have you ever felt frustrated or daunted when trying to help a struggling learner? We, the co-chairs of the STFM Group on Learners in Academic Difficulty, understand! And we want to help you experience the satisfaction of helping your learners reach their highest potential.
Below are key strategies that will help you assess and assist your own learners: motivational interviewing, creating a differential diagnosis for the behaviors, and developing target behaviors and plans. We also include cases, so read on to see how you can use these skills to work with:
- A resident who refuses to admit a patient
- An intern with disorganized presentations
- A senior resident who struggles to lead the team
Motivational Interviewing: A Tool for the Supportive Ear
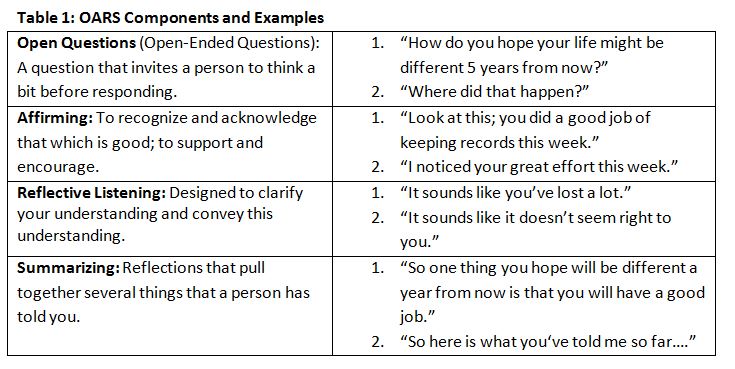
Learners in academic difficulty may feel ashamed and often judged by their teachers when it comes to feedback regarding their behaviors or overall academic performance. Motivational interviewing can offer the learner a more supportive ear. OARS is a motivational interviewing tool that requires more listening than talking, which at times is what the learner needs to feel supported.1
Case 1
An outpatient attending tells the resident on call for the family medicine inpatient service that he wants a patient admitted for a diabetic foot infection that did not respond to oral antibiotics. The resident, who took 20 minutes to return the attending’s initial page, reluctantly assesses the patient and then argues with the attending that the patient doesn’t need admission. Frustrated, the attending calls the resident’s inpatient faculty, who also assesses the patient and agrees with the need for admission and IV antibiotics. As the inpatient attending discusses the case with the resident, she begins to cry.
- Inpatient attending: This admission seems to be causing a lot of stress for you. Let’s talk about it briefly today and plan to discuss it more tomorrow. (O) What are your thoughts about your interaction with the outpatient attending?
- Resident: I am just exhausted. I’ve already had five admissions, and I don’t want to do any unnecessary admissions. This patient should do fine with oral antibiotics at home.
- Inpatient attending: (A) Wow, five admissions. You’ve already done a tremendous amount of work today. (R) What I’m hearing you say is that another admission would just put you over the top. Maybe that made you set the admission bar higher than it would be normally.
- Resident: Yes, I guess if I didn’t have as many other admissions I wouldn’t push back on this one so much. I feel bad that I got so frustrated.
- Inpatient attending: (S): Let’s summarize here. You have more work right now than you can safely manage. Since this patient hasn’t responded to oral antibiotics, we do need to admit her. How about you delegate some of your other tasks to me so that you can concentrate on this admission. And tomorrow, once you’ve had some rest, we can talk more about how to deal with similar situations in the future.
- The meeting went very well the next day. The resident stated that she felt supported. She expressed understanding regarding her unprofessional behavior, made a commitment to apologize to the outpatient attending, and agreed to give a lecture in morning report on Diabetic Foot Infection.
Generating a differential diagnosis
Just as one clinical symptom can be caused by many different underlying diseases, so the learner’s observed behavior can have various underlying causes. We need to diagnose the most likely cause and direct our treatment accordingly. The SOAP approach is an especially useful framework because it is so familiar to us from our clinical work and also helps standardize our thinking.2
Subjective: What made you think there might be a problem with this interaction? Ask what others think of this learner’s performance. Determine if a pattern of behavior exists.
Objective: Document specific instances. Be specific and behavioral in your description. (“Showed up late to clinic 3 days this week.” “Had the correct data for a patient with a COPD exacerbation but had difficulty synthesizing data to make an assessment.”)
- If others are raising the concerns, get as much specific, behaviorally based data from them as possible. Ask for written documentation.
Assessment: Generate a differential diagnosis.
- The six ACGME Core Competencies are a good place to start. Guerrasio expands these into 10 “competencies plus,” subdividing Patient Care and Communication and adding mental well-being.3
- Also consider: confidence, systems or environmental issues (eg, not given adequate orientation/expectations, challenging fit between learner and attending)
***Key point: When faculty colleagues come to us with concerns about a resident, they tend to assume that the underlying issue is a gap in medical knowledge or clinical synthesis. Very often we find that instead there is a difficulty with communication and/or confidence which, because it impacts clinical performance, appears to be a knowledge issue.
Plan: Decide on next steps.
- Diagnoses: Decide what other data you need to further refine your diagnoses.
- Ask other preceptors or staff for their input.
- Consider direct observation of patient encounters.
- Decide what you would like to ask the learner directly.
- Treatment: prioritize one domain at a time for intervention.
Positive reframing (ie, teaching = parenting)
Parenting books tell you that if you want to change your child’s behavior, tell your child what you want her to do rather than not do (eg, instead of “Stop whining!”, ask for what you want in a calm voice. The same is true in medical education! Decide what you want your learner to do or accomplish. This is the target behavior. Then choose strategies that will help your learner accomplish the target behaviors.

Case 2
An intern’s evaluations consistently mention that his presentations need to be more organized. One attending thinks that he is not taking enough time to prepare for rounds and needs to come in earlier.
- Differential diagnosis: organization/time management, clinical synthesis, communication.
- Initial diagnosis steps: When the intern is asked to reflect on the issue, he endorses that he knows in his head what he wants to say, but he can’t get the phrasing out the way he wants to and gets flustered.
- Refined differential diagnosis:
- Target behavior: present clinical data and management plans in a clear and organized manner.
- Strategies:
- Discuss methods to decrease presentation anxiety (eg, frequent practice, self-calming techniques such as deep breathing)
- Using a few known patients, practice presentations with audio recording, self-reflection, immediate feedback, and second practice.
- Outcome: presentation coherence improves over the next several rotations.
Case 3
Attendings come to you concerned that a senior resident is struggling to lead his inpatient team. He has trouble making decisions on rounds. One attending asks him on rounds to choose an antibiotic for a common infection, and he is unable. The attending thinks that he does not have a sufficient fund of knowledge to lead the team safely.
- Differential diagnosis: medical knowledge, clinical synthesis, communication, confidence, organization, mental well-being.
- Initial diagnosis steps: the resident’s In-Training Exam scores are average for his year. When the resident is asked to reflect on the issue, he endorses that he knows the answers but is worried about being wrong and therefore doesn’t commit to a management plan. It’s easier for him to come up with a plan after having some time to think about it and look up the answer to confirm it.
- Refined differential diagnosis: communication and confidence.
- Target behavior: Make clinical decisions at the point of care quickly and decisively.
- Strategies:
- Discuss his expectations of his own learners: would he rather his interns make a wrong clinical decision or make no clinical decision at all? Help him extrapolate this to his own situation.
- Reflect on barriers to accessing knowledge quickly and making decisions quickly, strategize ways to improve these skills.
- Role play cases with the objective to quickly decide on management plans.
- Outcome: Confidence improved after sessions, able to lead inpatient team and make on-the-spot decisions more easily.
We hope that you will be able to incorporate these skills into your own practice and experience the satisfaction of helping your learners reach their highest potential. Let us know in the comments of this blog post other advice you would give to help learners. Have a question about our advice? Put it in the comments, and we’ll get back to you.
References:
- Miller WR, Rollnick S. Motivational interviewing, helping people change, third edition. New York: Guilford Press, 2013.
- Guerrasio J. Remediation of the struggling medical learner. LaVergne, TN: Lightning Source, 2013.
- Langlois JP, Thach ST. Managing the difficult learning situation. Fam Med 2000;32(5):307-9.

Excellent. Keep these coming!